


“What is in it for you? Why are you doing this?” asks one of the Health Navigators (HNs) in Channapatna, the “Toy-City” of Karnataka, back in 2016 during Design Beku’s first visit. As designers, they definitely wanted to understand the work of health navigators but were more interested in learning how to work with the HNs to enable digital technology to become a part of their work-life. These inputs were important because their first engagement’s focus was to make interactions between the health navigators and the clients meaningful and address the issues of non-communicable diseases such as hypertension, diabetes mellitus, malnutrition, and general well-being.
Health navigators are a group of mainly women from the local community who are trained and supported by MAYA Health as community health workers. These health workers are trained to offer services for testing and management of chronic health conditions such as diabetes, hypertension, and malnutrition within their communities. Through this, they earn their livelihood and also ensure healthy communities.
Since 2016, Design Beku, a Bengaluru-based design and technology collective, and Movement For Alternatives And Youth Awareness (MAYA), a Karnataka-based non-governmental organisation working to create an empowered and equitable society that systematically addresses livelihood, education and health, are working together to design and develop support infrastructure for and with the health navigators.

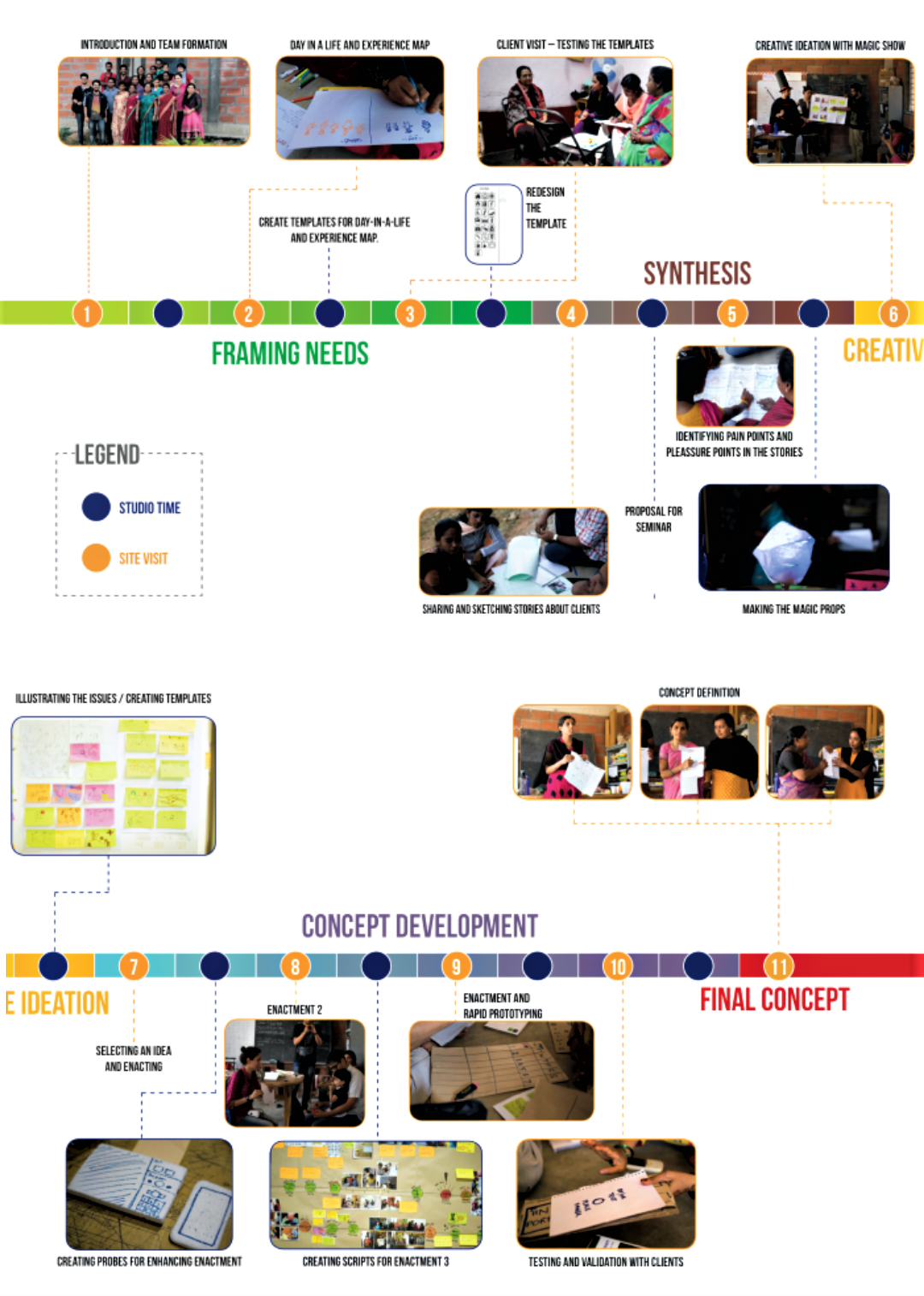
Following the visit, for the first pilot project Design Beku chose to focus on participatory design and learning about Human-Centred Design (HCD) to improve the communication between health navigators and the community. Through a 14-week project, Design Beku along with students of Srishti Institute of Art, Design & Technology, worked closely with the health navigators of Channapatna.
We are increasingly seeing the use of the Human-Centred Design (HCD) approach—the development of mobile applications and digital means of data collection and dissemination. HCD is now a common feature driving the design, development and deployment of digital-technological solutions aimed to address problems affecting public goods such as education, poverty, heritage, and healthcare and hygiene. Adoption of HCD for public goods has largely been pushed by global philanthropic forces, like the USAID and Bill & Melinda Gates Foundation, who find their presence in India too, as well as government entities and the private sector.
While HCD is readily used in corporate contexts, it has also been troublingly embraced by the development sector as it is considered an easy to use tool to further mandates of organisations, despite the ideological contradictions of using this approach in spaces that should privilege lived experience, local knowledge and expertise. The idea that designers who often come from spaces of privilege, be that of caste, gender, and/or race, can fully empathise with the lived experiences of myriad communities of users, is an audacious one, as well as presumptuous. The time and care given to developing solutions along with the health workers in Channapatna ensured that every stakeholder in the process is valued and taken into consideration.
Seeking Solutions by Designing Collaboratively
Following this pilot project, Design Beku and MAYA Health decided to further develop one of the ideas conceptualised by the health navigators—mapping the food habits of each household to plan a healthier diet plan with the health of tablet/smartphone application. This time, students of Srishti Institute and IIIT-Bangalore worked with the same teams of health navigators for conceptualising and designing an App. The App was intended to work on the handheld tablets the health navigators use with an aim of collaborative prototyping and testing in the local setting.
The team envisioned a practice where the health navigators visited the client’s house, and through mapping, a day-in-a-life of the client’s household captured the data about food cooked and consumed in the past 24 hours. This data is captured on the tablet’s App, which visualises it in the form of a thali [a plate of food].
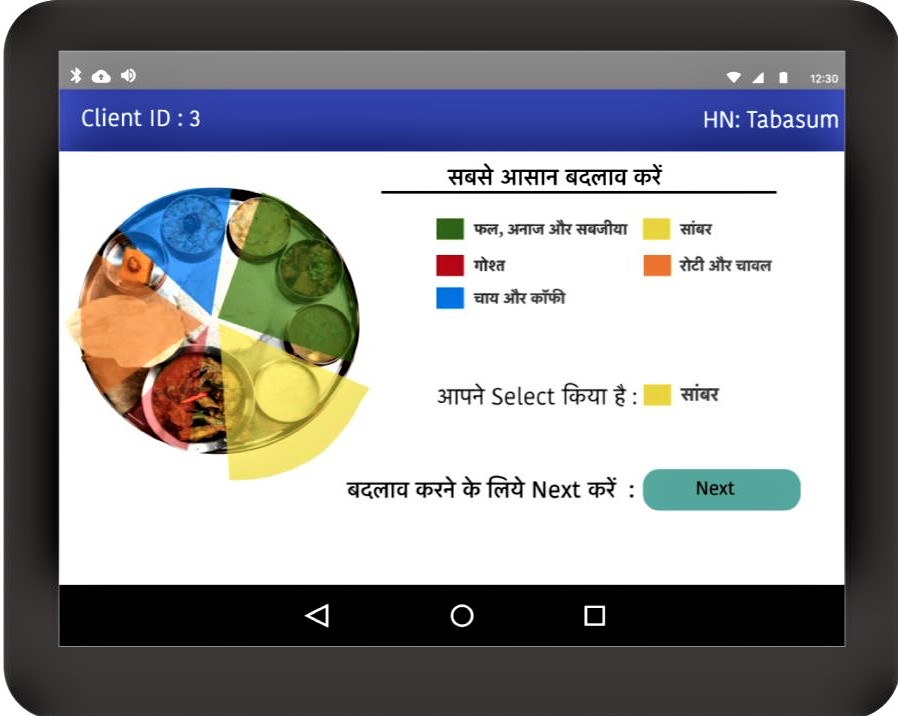
Rather than showing the nutrients or calorie values, the food is categorised into directly relatable categories—rice and rotis, meat, sambhar and curries, milk and curd, coffee and tea—which are colour coded. Both, the health navigator and the client, discuss and move the lines on the interface to decide which should be an “ideal” diet for the client. But the ideal is not to be followed, immediately at least, and rather the client chooses to reduce or replace one item of food that they consider to be harmful in consultation with the health navigator. They can either reduce the frequency or the size of consumption. The health navigator, the client and their family then together track this, in a way to open up periodic discussions about challenges faced in what the client has decided to cut down on.
At that time, we thought that this vision of collaborative diet planning supported by an interactive App was quite departing from all the mainstream applications. Usually, the applications for diet and nutrition planning for people with diabetes and hypertension focus on “calories count” alone.

The next step involved coding a simple mock-up of the App based on the roleplaying sessions between the health navigators with their clients. Well, coding isn’t particularly easy especially when no two humans are the same and realities differ significantly. Consider the following vignette from one of the sessions with an elderly woman.
The setting is a living-cum-bedroom of a 60 year-old-woman client. She is a patient with hypertension and diabetes. Along with the client is her husband, and also present in the room are the health navigator, design students and DB team who are working on the design. The health navigator begins the session in Urdu by explaining the idea behind this session and invites the elderly women to join in. The health navigator opens the App on her tablet and maps the daily food intake of the household based on the inputs provided by the couple.
The discussion then moves towards an ‘ideal’ diet, and the couple unanimously shares that they should be eating more fruits and leafy vegetables, and reducing red-meat and fatty foods. They are nodding their heads at what they (and all of us) have learnt about healthy diets in general.
When it is the time to decide what food item, in particular, would the elderly woman like to reduce or replace from her diet, there’s a look that appears when a vexed question is posed. The woman shared that thrice a week she cooks kheema-ball curry, which is eaten during lunch and dinner during the three days. “I know It is quite bad for my health and I want to reduce the intake of red meat,” she says. The health navigator asks if she could reduce the intake to twice a week? The elderly woman replies with a “No”. Could she eat the kheema-ball curry only for lunch? “No, not possible. I need to feel the taste of the meat and curry to have a good night’s sleep,” says the woman. Worrying that no fruitful outcome will yield from this discussion, the health navigator asks. “How many meatballs do you eat during each meal?” The woman says she eats two. “Could you reduce it to one keema-ball per meal?” asks the health navigator. “No, I like to have two,” says the woman. The health navigator patiently follows up by asking, “What is the size of these balls, narangi ya nimbu [an orange or a lemon]?” The woman replies, “narangi”. The health navigator, with a smile on her face, asks, “could you make the kheema-meat balls the size of a nimbu?” “Yes!” replies the woman.
Finally! During this entire discussion, the health navigator’s tablet with the App is in the background.
Addressing Health and Nutrition by Putting People First
This experience of enacting the possible practice of a collaborative diet and food habit formation between a health navigator and her client’s household, impelled the team to rethink its earlier understanding of how radical and different a vision they had. The vision of collaborative diet and food-habit forming that emerged in this session was ever more radical, opening up for critical questioning of all the assumptions about food, diet and data they had built in the design of the App and the activity it aimed to support. What emerged was an imagination to capture the irony—where there are no predetermined standards of ‘right’ food, be it quantity, quality or ![]() nutrition levels; what is good and ideal emerges out of an ongoing and collective tinkering, and taking advantage of the particular socio-material settings of the practice. Such an approach to design and technology helps foster a practice of care. Unlike the kind of technological imaginations of surveillance, datafication and enumeration being pushed on to the frontline health workers in India in the name of digital health through Apps such as the Poshan Tracker.
nutrition levels; what is good and ideal emerges out of an ongoing and collective tinkering, and taking advantage of the particular socio-material settings of the practice. Such an approach to design and technology helps foster a practice of care. Unlike the kind of technological imaginations of surveillance, datafication and enumeration being pushed on to the frontline health workers in India in the name of digital health through Apps such as the Poshan Tracker.
According to the National Family Health Survey (NFHS) 2019-21, India’s population has not witnessed any significant improvement in health and nutrition. In particular, the areas where India has performed poorly are maternal anaemia, stunting, obesity, wasting, and breastfeeding. The COVID-19 pandemic has only made this worse. In such a scenario, there’s a need to address this health crisis, especially for vulnerable communities in India. “At the current rate of progress, the global nutrition targets will not be achieved by 2025,” states the Global Nutrition Report 2021. With this complex and herculean task ahead, India needs to find solutions and efficiently implement the existing ones to improve its health and nutritional status and meet global goals.
Designing with Care
Engagements with development sites are usually time-bound projects, but since Design Beku’s first visit in 2016 what emerges is an example that shows us how design could be approached as care-in-practice. The original goal of developing Information Education Communication (IEC) Materials to engage with the community members in better management of diabetes and malnutrition is now complemented by a protocol and format for data collection and storage as part of the COVID-19 response by MAYA Health. During COVID-19, the health navigators have served as Community COVID Companion to ensure their communities are not neglected or affected.
By using a combination of handwritten records, phone calls, and WhatsApp, Design Beku continues to work with the health navigators to collaboratively archive local health knowledge through a community-owned Wi-Fi mesh network. Wi-Fi mesh networks are a form of decentralised information and communication networks providing viable access for local-wireless creation and sharing of digital content. During the pandemic, the health navigators and the teams involved have arrived at a collective understanding of the value and importance of local health knowledge and know-how.
I did not know that we have so many resources in our area [Channapatna] about COVID-19 and its experiences!
—Ramakka, Field Coordinator, MAYA Health
The collaboration has also given the health navigators an opportunity to work as researchers to understand the experiences of pregnant women and their families in accessing healthcare infrastructures in Channapatna. They can now speculate on creative design solutions to address the challenges. This has helped everyone involved gain a deeper understanding of both the larger issues of public and community health and the role of digital technology in public health. Working closely with the health navigators has provided an intimate understanding of their lives and lived experiences. In turn, the health navigators got a chance to see the lives of all those working on this project, their motivations and experiences. The outcome being all of us gain mutual understanding and the experience of working together to design digital technological support for their work.
For Design Beku, designing inherently means building long-standing relationships of care, and with care, with the people who will be most impacted with the results of the technology that gets designed. Since October 2021, they are working with Janastu, and 11 of the 90 health navigators and one of the coordinators in Channapatna with an overall ambition to set up a community wifi mesh network-enabled feminist server and infrastructure to enable participatory archive of locally rooted and relevant health knowledge, as well as collaboratively build the archive.

The Future of Design and Technology in India
This experience has reinforced Design Beku’s commitment in its work to “explore how technology and design can be decolonial, local and ethical. And work with contexts and collaborators; not clients.” From rejecting the focus on understanding as a way to empathise as a way to design solutions, the team now views empathising as a way to form and sustain any human relationship. But we need to understand that long term, sustainable change needs much much more than empathy, and certainly not empathy that is “at scale”.
A typical HCD process lays emphasis on understanding the end-user (the human) through activities of ‘immersion’ that leads to understanding and empathising with the end-user and their needs and requirements, which will then be coded into the design solution in a creative manner. However, through the journey of health navigators in Channapatna, we see a first-hand glimpse of how an emphasis on understanding the end-users and their lives inherently means pouring in a lot of resources and time to getting the design team to understand the lived everyday life and the underlying development contexts, something which individuals and communities (of end-users) are already experts of.
Users and their contexts are not a precursor for design, but an evolving outcome for a process of collaborative and situated engagement with people and their realities. This necessitates us shifting our approach from the idea of empathy to that of an ethics of care. The feminist principle of care holds at its centre the notion that there is an ethical imperative to create spaces that allow for care to be generated for and practised by those who inhabit those spaces. Care is seen as a form of situated and collective action of tinkering with possibilities for a just, inclusive and equitable life.
The story of India’s health and nutrition is a complex one and the response to it by the current imperatives of big tech, be it governmental or corporate, is being facilitated in the opposite direction. By using design and technology as a weapon to surveil and harass its users, entities continue to turn this plight into profit.
This article is the first instalment of our series on introducing design, technology and development.
Featured image of health navigators, Noor and Shabeena, along with student Chakkaravarthy presenting their concept for data-driven interaction with a client from the community | Photo courtesy: Design Beku


